FIRST AID ESSENTIALS
DRSABCD
Here we are looking at the first aid acronym known as DRSABCD.
This is the basic life support flow and should be used in all cases:
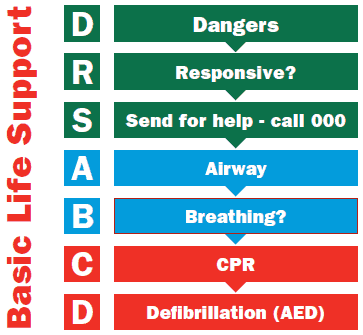
Dangers
- Quickly assess the situation and environment by observing, listening and using your sense of smell
- Identify any potential dangers that could impact the safety of the casualty, bystanders or yourself
- Conspicuous dangers could include; traffic, people, animals, fire, explosions, hot oil, slip/trip hazards, etc.
- Inconspicuous dangers could include; Gases, electricity, pets, mental health, drug reactions, etc.
- Keep looking for dangers as this scenario can change from safe to unsafe very quickly
- Remove children to a safe place in the event of a scenario for their psychological well being
- If it is not safe to proceed, call for help.
REMEMBER, you come first at an accident scene – if in danger remove yourself
Responsive
Check for a response using talk and touch or the C.O.W.S method:
- Can you hear me?
- Open your eyes
- What’s your name?
- Squeeze my hand
Individuals who are unresponsive but breathing normally should be positioned into a side-lying recovery position. The recovery position is a lateral, side-lying recovery (lateral recumbent) position as shown below.
To place into recovery position (1 person):
- Lay casualty on their back
- Place the casualties closest arm to you across their other shoulder (this arm can act as a pillow to the cheek) with the far arm out or up
- Place the casualties closest knee bent up by placing hand on ankle and under knee
- Hold the casualties knee and shoulder and roll them away from you
- Make sure the top leg acts as an anchor to prevent patient from rolling further.
If the person is unconscious:
- Ensure the safety of both the person and rescuer
- Place the person on the ground and position them on the side. Ensure their airway is open.
- Call an ambulance.
- Promptly stop any bleeding.
- Constantly re-check the person’s condition for any change.
- Ideally, the most experienced rescuer should stay with the person.
When moving an unconscious casualty;
- Care of the airway takes precedence over any injury, including the possibility of a spinal injury.
- Every effort should be made to avoid any twisting or forward movement of the head and spine.
- Who is breathing normally should be positioned into a lateral, side-lying recovery position.
REMEMBER, if more than one person requires attention, the care of an unconscious person has priority.

Send for help
Calling for help requires careful consideration based in each situation and the severity. Ask yourself:
- Is this a critical or serious incident?
- Is breathing compromised; is the bleeding severe, are they suffering from a serious condition such as (but not limited to) cardiac arrest, stroke, anaphylaxis, severe asthma.
If yes; you need to call Triple Zero (000).
If it is a minor injury that can be managed using first aid techniques, carry out the required first aid and suggest the person seeks medical advice if warranted e.g. minor burns or a sprain etc.
If in doubt – call your management team, but in serious cases – do not delay in getting emergency help!
Airway
Airway management is required to provide an open airway when a person is unconscious, has an obstructed airway, or needs rescue breathing.
In an unconscious person, care of the airway takes precedence over any injury, including the possibility of spinal injury.
To assess breathing and airway, leave the person in the position in which they have been found, unless fluid or matter obstructs the airway.
To clear the airway the mouth should be opened and the head turned slightly downwards to allow any obvious foreign material (e.g. food, vomit, blood and secretions) to drain.
If the airway becomes compromised during resuscitation, promptly roll the person onto their side to clear the airway. Once the airway is clear, reassess for responsiveness and normal breathing. Begin resuscitation as appropriate
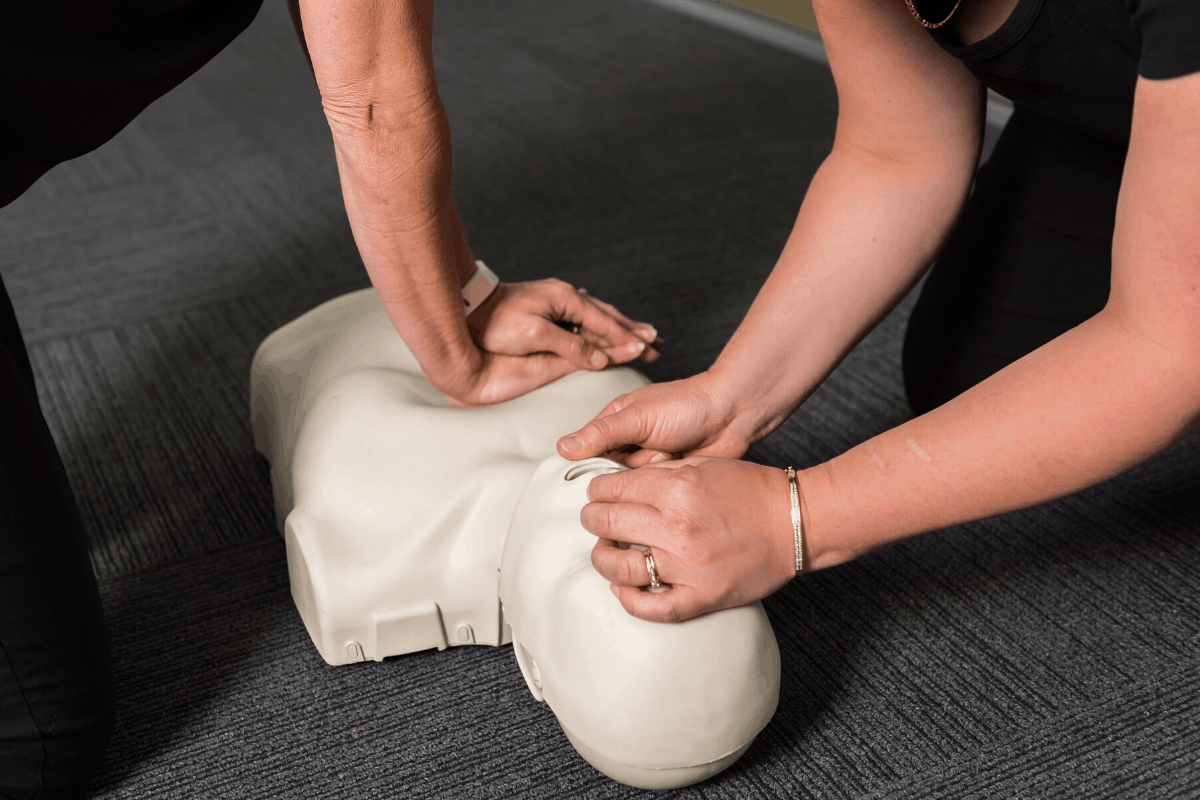
For an unresponsive adult or child, open the airway using the head tilt-chin lift.
Head tilt/Chin lift
- One hand is placed on the forehead or the top of the head.
- The other hand is used to provide chin lift.
- The head (NOT the neck) is tilted backwards .
- For an infant, open the airway by placing the head in the neutral position and support the jaw from falling back.
It is important to avoid excessive force, especially where neck injury is suspected.
When the person is on their side, the head will usually remain in this position when the rescuer’s hands are withdrawn.

Breathing
Check for breathing using look, listen and feel.
- LOOK for movement of the upper abdomen or lower chest
- LISTEN for the escape of air from nose and mouth
- FEEL for movement of the chest
Breathing may be absent or ineffective as a result of:
- Direct depression of, or damage to, the breathing control centre of the brain
- Upper airway obstruction
- Paralysis or impairment of the nerves and/or muscles of breathing
- Problems affecting the lungs
- Drowning
- Suffocation.
If an unconscious person is unresponsive and not breathing normally after the airway has been opened and cleared, the rescuer must immediately begin chest compressions and then rescue breathing.
CPR
All rescuers should perform chest compressions for all those who are unresponsive and not breathing normally.
Commence CPR by giving 30 chest compressions followed by two breaths (ratio of 30:2).
CPR Technique
- Palm or “heel” of the hand should be placed directly in the centre of the chest ideally on the lower half of the sternum. (between the nipple or armpit lining) avoid compressing too low or too high.
- Compressions should be rhythmic and consistent, avoiding rocking back and forth or quick jabs. Rescuer should allow equal recoil of the chest to depth compressed.
- 100-120 beats per minute (bpm) is the recommended compression rate range. There is evidence to suggest that compression rates below 100bpm or above 140bpm lead to lower survival rates. (closest to 100bpm is best). You can sing songs in your head i.e. 2 choruses of row, row, row your boat / stayin’ alive.
- Compression should be 1/3rd the depth of the chest
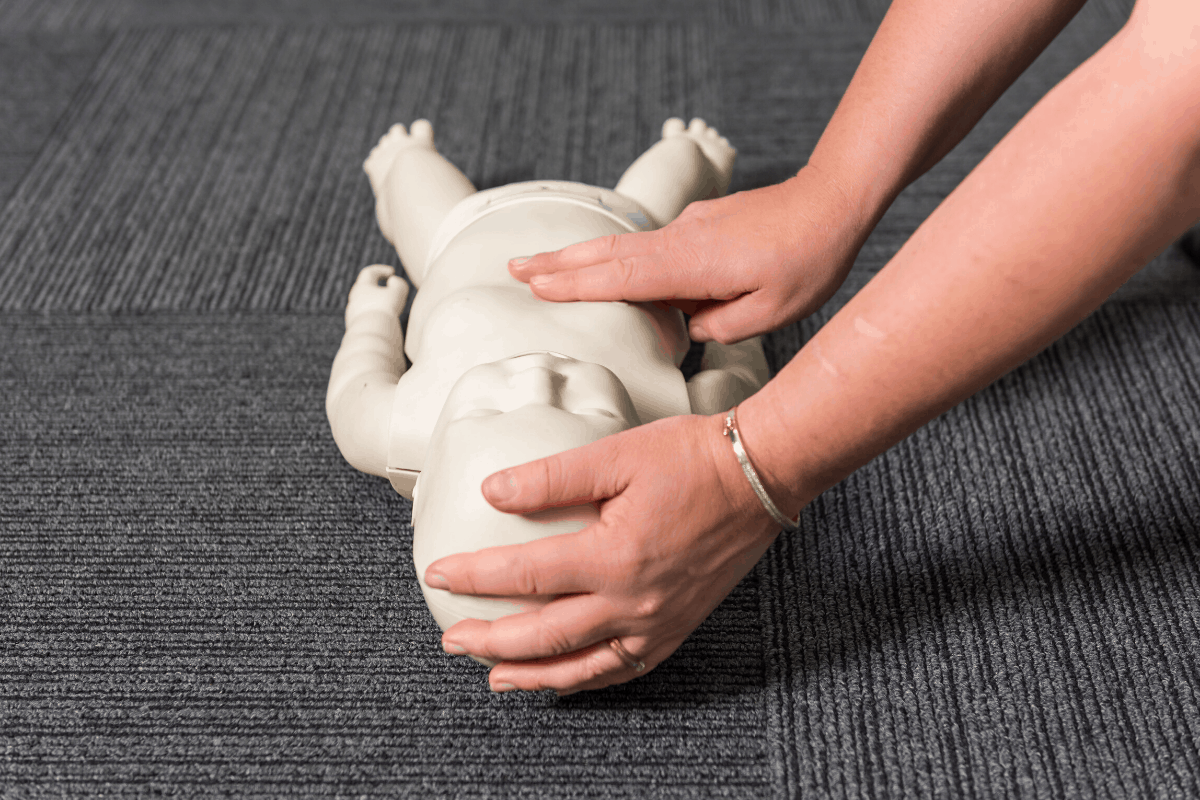
- The correct compression technique for:
- infants (0-1 years old) is 2 fingers
- children (1 – 8 years old) is 1 hand
- children and adults (8 years and above) is 2 hands interlocked
Tips when providing CPR:
- To a pregnant casualty, remember to elevate right hip to promote blood flow through the body.
- Keep going until medical help arrives, until you are unable to continue, until a danger presents itself, until a doctor pronounces the person deceased or until they show signs of life.
- Rib fractures and other injuries are common but acceptable consequences of CPR given the alternative of death. There is a higher value of survival benefit of CPR against the risk of other injury caused by layperson CPR delivery.
- Bystander CPR should be actively encouraged for assistance
- Where there are multiple rescuers available, always ensure that required equipment has been obtained e.g. AED, pocket mask etc. and that they are in charge of liaising with the ambulance.
Defibrillation
Attach an Automated External Defibrillator (AED) as soon as possible and follow the prompts.
CPR alone will not save a person who is in VF (Ventricular Fibrillation). A defibrillator shock combined with effective CPR delivery allows for the possibility of survival. An AED applies an electric shock to the body to enable the heart rate to go back into a normal rhythm from an abnormal rhythm.
- Pads are placed in specific places for adults: both on chest
- Pads are placed differently for Children 1-8: one on front and one on back
- Pad placement is to ensure a shock is delivered on an axis through the heart. Pads must not be touching and should be ideally placed at least 8cm apart to avoid arcing between the pads.
- Ensuring that an AED is placed to the correct setting whether it be paediatric or adult depending on casualty age. If paediatric options are not available it is reasonable to go ahead with adult pads.
- Ensure that all parties are away from the person receiving the defibrillation shock.
- Chance of survival decreases by 10% every minute taken until Defibrillation due to Ventricular Fibrillation (“VF” shaking/quivering of the walls of the ventricles”) e.g. 90% survival rate after 1 minute

ARC Guidelines and Related Links
ANZCOR Guideline 2 – Managing an Emergency
ANZCOR Guideline 3 – Recognition and First Aid Management of the Unconscious Victim
ANZCOR Guideline 5 – Breathing
ANZCOR Guideline 6 – Compressions
ANZCOR Guideline 7 – External Automated Defibrillation in Basic Life Support